Unilateral Oculomotor Nerve Palsy as a Rare Manifestation of Isolated Pre-Communicating Segment of Posterior Cerebral Artery Thrombosis
Article information

Abstract
Ipsilateral mydriasis (IM) is usually not acute. However, the acute occurrence of unilateral dilated pupil may result in acute ischemic stroke. Herein, we present 3 patients with IM, lateral eye deviation, ptosis, and contralateral hemiparesis due to isolated occlusion of the pre-communicating segment of the posterior cerebral artery with preservation of the posterior communicating artery, which was successfully treated by emergent mechanical thrombectomy. In a 3-month follow-up, all patients were independent without any neurological deficits.
INTRODUCTION
Common etiologies of unilateral cranial oculomotor nerve (CN III) palsy are diabetes, aneurysmal compression, and cerebral tumors. A rare cause of CN III palsy is cerebral ischemia, due to isolated P1 occlusion.
Herein, we report 3 cases of ipsilateral mydriasis (IM) and hemiparesis due to thrombosis of the short pre-communicating (P1) segment of the posterior cerebral artery (PCA).
CASE SERIES
Patient 1
A patient in their 50s presented with tonic-colonic seizure due to a basal ganglia hematoma. Diagnostic cerebral angiography was performed and did not reveal any vascular abnormalities. After 15 minutes in the recovery room, the patient experienced left mydriasis, ptosis, lateral deviation of the left eye and right arm paresis (National Institutes of Health Stroke Scale, NIHSS=2). While the computed tomography (CT)-scan did not show new intracranial hemorrhage (ICH) or expansion, magnetic resonance imaging (MRI) revealed a small ischemia in the left peduncle and left thalamus. New cerebral angiography showed a left isolated P1 occlusion while the left PCA was supplied by the left posterior communicating (PCOM) artery. Mechanical thrombectomy of the left P1 was performed with the stentrieval technique. After the first attempt, the left P1 was completely opened, achieving a thrombolysis in cerebral infarction (TICI) of 2b (Fig. 1). After 24 hours, the patient improved except for mild ptosis of the left eye and slight diplopia. Subsequently, 100 mg of aspirin and 75 mg of clopidogrel were prescribed for the patient. On day 5, the patient was discharged with a modified Rankin scale (mRS) of 0.

Patient 1. (A) Cerebral angiogram shows left isolated pre-communicating (P1) occlusion (black arrowhead). (B) Ipsilateral internal carotid artery injection shows post-communicating posterior cerebral artery (PCA) filling by the left posterior communicating artery. (C) Post-thrombectomy angiogram shows patent P1 and PCA.
Patient 2
An adult patient was admitted for endovascular treatment (EVT) of a basilar tip aneurysm. The patient had a history of seizures and right frontal large arteriovenous malformation. Arteriovenous malformation was ruptured twice and has been treated with 5 sessions of EVT. The basilar tip aneurysm was 7.5×6.5 mm in size with a neck of 5.2 mm. The aneurysm was completely secured by balloon-assisted coiling by inflation of a balloon Scepter C 4×20 (MicroVention) in the tip of the basilar artery and left P1. In the recovery room, the patient did not wake up appropriately, and the physical exam showed left eye mydriasis, ptosis, lateral deviation of the left eye with right slight hemiparesis, and slight confusion (NIHSS=10). The CT-scan ruled out any ICH. A new cerebral angiogram revealed left isolated P1 thrombosis. The left PCA was supplied by the left PCOM artery. Mechanical thrombectomy was done by thrombosuction, achieving complete opening of the left P1 (TICI 2b). Then, 15 mg of Eptifibatide was also injected in the left PCA. In the recovery room, the patient became alert and left mydriasis resolved. The next day, she had a NIHSS of 4 and was discharged on day 5 without any neurological deficit (mRS 1). At 3-month follow-up she had a mRS of 1 (Fig. 2).

Patient 2. (A) Post-operative angiography reveals isolated left pre-communicating (P1) occlusion in vertebral injection (black arrowhead). (B) Ipsilateral internal carotid artery injection shows post-communicating posterior cerebral artery (PCA) filling by left posterior communicating artery. (C) Post-thrombectomy angiogram shows patent P1 and PCA in vertebral injection.
Patient 3
An adult patient presented with vertigo, nausea, and vomiting. The patient had a history of hypertension and diabetes mellitus. On admission, the blood pressure was at 170/90 mmHg. After 6 hours of observation, the patient developed left hemiplegia, right mydriasis, ptosis, and lateral deviation of the right eye with a NIHSS of 8. Emergent MRI showed right isolated P1 occlusion. Cerebral angiography revealed right P1 thrombosis and a partial thrombosis of the basilar tip aneurysm. Mechanical thrombectomy was performed using the stentrieval technique, achieving TICI 3 (Fig. 3). After 24 hours, the patient became alert and showed improvement of hemiparesis, vertigo, and double vision, except for right eye mydriasis and lateral deviation. Echocardiography was normal and the cause of the embolic stroke was not elucidated. The patient was discharged with a mRS of 1. After 3 months, the mRS was 1 with complete improvement of the right CN III palsy.

Patient 3. (A) Initial vertebral injection angiogram shows right pre-communicating segment occlusion (black arrowhead). (B) Right carotidal injection shows the right posterior communicating (PCOM) artery. (C) Right vertebral injection also demonstrates patent basilar artery and PCOM artery.
DISCUSSION
We report 3 cases of acute CN III palsy due to acute stroke following isolated occlusion of the P1 segment of the PCA (Fig. 4). In addition to the CN III palsy, the patients had other symptoms of acute stroke, which were mild in 1 patient and more prominent in 2 patients. As the perfusion of the tip of basilar artery and post-communicating PCA were preserved by patent basilar artery and PCOM artery, the visual and motor symptoms were not very prominent in our patients.
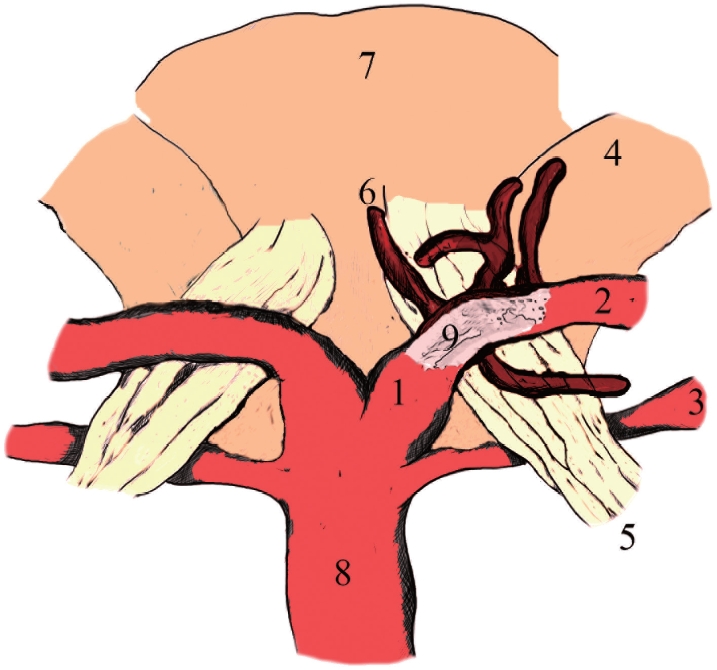
The illustration shows the pre-communicating (P1) segment of posterior cerebral artery branches (thalamoperforating arteries) supplying the oculomotor nerve. The occlusion of the P1 could affect the arterial supply of the oculomotor nerve in acute ischemic stroke. 1, P1 segment; 2, P2 anterior segment; 3, superior cerebellar artery; 4, cerebellar peduncle; 5, oculomotor nerve; 6, thalamoperforating arteries; 7, mesencephalon; 8, basilar artery; 9, a clot in the P1 segment.
Oculomotor nerve palsy is usually non-acute and a consequence of cerebral tumors, microvasculature disease, compression effect of an aneurysm, and dural arteriovenous fistula [1]. Acute onset of unilateral CN III palsy is usually attributed to traumatic brain injury and hemorrhagic complications. In patients with previous cranial surgery or in the presence of an intracranial space-occupying lesion, early onset of mydriasis may be alarming with increased intracranial hypertension and an early sign of cerebral herniation due to new ICH and expansion of previous hematoma [2]. In our first 2 patients, we expected a rapidly expanding ICH following EVT with observation of unilateral mydriasis. Therefore, we performed a CT scan as the first step to rule out ICH.
While unilateral CN III palsy could occur in the setting of malignant middle cerebral ischemia due to cerebral herniation [3], it is rarely reported in the acute phase of ischemic stroke [4,5]. Unilateral CN III palsy is an atypical presentation of P1 segment thrombosis [5]. Usually, patients with P1 ischemic stroke present with hemiparesis, sensory loss, and visual problems [6,7], as P1 perforating branches supply cerebral peduncles, tegmentum, and geniculate bodies, colliculi, and pulvinar of thalamus [8]. Blood supplies of the proximal part of the third cranial nerve could explain CN III palsy following an isolated P1 segment. The proximal cisternal part of the third cranial nerve supplies by thalamoperforating branches of the P1 segment and the supplies of the distal cisternal part originate from the P2 segment [8,9]. The cavernous part of the CN III is supplied by the inferolateral and meningohypophyseal trunk of the internal carotid artery and superior orbital artery [8-10].
All our 3 patients significantly responded to mechanical thrombectomy, and their symptoms, including CN III palsy, were resolved with the reperfusion of P1. Recently, Voss et al. [5] reported a case of unilateral isolated P1 occlusion presenting with vertigo and CN III palsy (NIHSS=1) that was treated with mechanical thrombectomy, leading to the resolution of symptoms. During angiography, the occluded P1 could be easily mistaken as hypoplastic or aplastic P1 when a prominent PCOM artery supplies the PCA and the perfusion of post-communicating PCA is well preserved. Therefore, the operators could easily hesitate to perform mechanical thrombectomy. However, a prompt decision could be made according to the symptoms of patients, including unilateral mydriasis and hemiparesis, and the imaging.
These cases demonstrate that unilateral mydriasis and CN III palsy could be the prominent presentation of a P1 ischemic stroke, while other symptoms could be mild. Therefore, it could be easily mistaken for an intracranial occupying mass lesion. Appropriate imaging, including MRI and CT angiography, could rule out other causes and reveal ischemic stroke and a P1 occlusion. Rapid mechanical thrombectomy can restore the perfusion of P1 and resolve the symptoms.
Notes
Fund
None.
Ethics Statement
Informed consent was obtained from patients. The ethical committee of Mashhad University of Medical Sciences approved the study and the code is IR.MUMS.REC.1401.139. We anonymized the patient information, such as sex and age, which could identify the patient.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: HB. Data collection: FQMS, SN, HP, and HO. Writing the article: FQMS and HB. Critical revision of the article: FQMS and HB. Final approval of the article: FQMS, SN, HP, and HO. Overall responsibility: HB.